




In this section
Short Term Side Effects
- General Effects
- Cutaneous (Skin) Effects
- Soft Tissue (breast) Effects
- Musculoskeletal Effects
- Gastrointestinal Effects
Long Term Side Effects
Side effects from treatment are typically divided into short term and long term side effects. Short term side effects are those that typically develop either during (within 1-2 weeks of starting treatment) or shortly after completion of the radiation therapy course. These side effects are also commonly short lived, and resolve within weeks (up to 3 months) after therapy completion. In contrast, long term side effects are those that develop at least 3 months after completing radiotherapy but occasionally can develop years after treatment. These side effects are often longer lasting and sometimes permanent.
This is a visual side effects chart showing short and long term side effects. Larger bubbles show higher likelihood of occurrence. To see a larger version, click on the chart.
Please note, this list does not represent all of the possible side effects you may experience during your radiation treatment course. Before treatment begins, ask your doctor about possible side effects and how best to manage them.
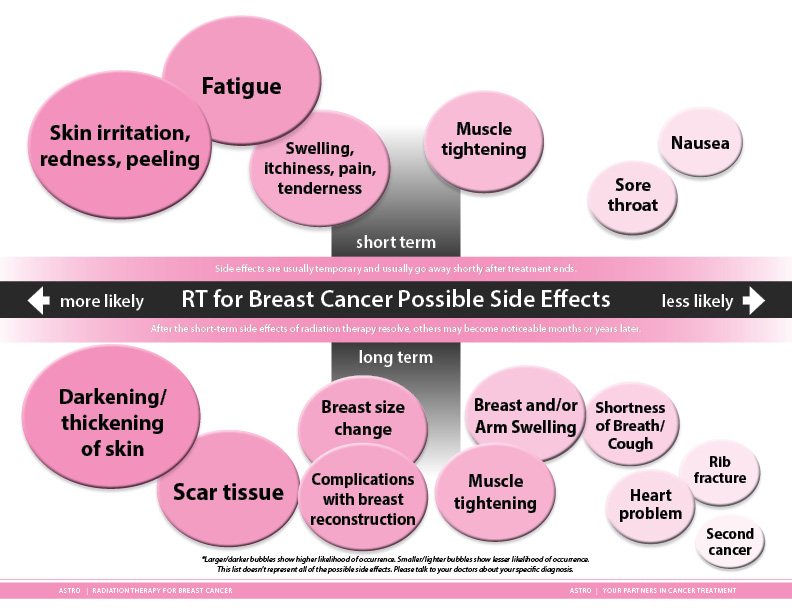
For patients who prefer to look at the side effects in text instead of graphics, please see below.
Short term side effects
- Fatigue (more likely)
Fatigue among patients receiving radiation therapy is commonly experienced as physical or mental tiredness that impacts one’s daily functioning and is beyond what one might expect from their normal activity levels. Fatigue is often cited as the most common side effect from cancer treatment and the reasons why patients experience fatigue with radiation therapy are largely unknown. Symptoms often start subtly but progress as radiation therapy continues. Fatigue often peaks near the end of therapy or shortly afterwards and can also continue for months even after radiation therapy is complete. Contributing factors to radiation treatment related fatigue during treatment may include poor appetite and/or nutritional intake, poor sleep habits and hygiene, comorbid conditions, and medications.
Patients often manage fatigue by getting extra rest throughout the day, getting adequate rest at night, eating a balanced diet, and pacing their activities. Maximizing your sleep may involve improving your sleep hygiene, which may include limiting caffeine and alcohol intake and limiting electronic screens close to your bedtime. Additionally, mild to moderate exercise can also help improve symptoms of fatigue, such as taking a short walk each day. Exercise, however, must be balanced with appropriate rest to be maximally effective.
Fatigue must also be distinguished from other medical problems that may have similar symptoms, such as depression, lung and heart issues, liver and/or kidney problems, or diabetes. Please review your symptoms with your radiation oncology team to determine what may be causing your symptoms and which interventions might be right for you.
- Skin irritation, redness, peeling (more likely)
As radiation is delivered to your body with external radiation, it typically travels through your skin to get to the areas that require treatment. In some cases, the skin itself is a target for the radiation, in an attempt to reduce the risk that the cancer returns. Therefore, when radiation is used, the radiation can cause the skin itself to be affected. When receiving radiation for breast cancer, the area of skin being exposed to radiation includes the breast and/or chest wall and, in selected cases, the skin over the shoulder and upper back.
The intensity of the potential side effects depends on the type of radiation you’re receiving, the area of the body being treated, and differences in the sensitivity of one’s skin. The radiation can cause irritation at any area exposed to radiation, but the most likely areas include those at the inferior breast, along the lateral breast towards the side of the chest, and along the upper chest and above the clavicle. Other areas that can have increased irritation include areas where one’s shirt or bra rubs against the skin, including the armpit and underneath the breast.
The radiation reaction develops over the course of the radiation treatment. Typically, patients do not notice much of a change during the first week of treatment, but can notice early skin changes during the second or third week. These early skin changes include the skin becoming more red, getting more dry, and feeling more irritated, sensitive to touch, and sometimes even painful. As the radiation progresses further, you may also notice skin darkening and flaking and/or peeling of the skin. When the skin peels, it can be dry and flaky or it can be moist and even drain fluid. Sometimes, these changes can happen within 1-2 weeks of radiation completion, and may take up to a month or more to heal afterwards. Darkening of the skin can last several months to years after the radiation is complete.
During the radiation course, talk to your radiation oncologist about how to manage your skin, as there can be many subtle differences in your radiation that may affect how it impacts your skin. In general, patients are given non-prescription topical lotions to help moisturize the skin and slow the progression of radiation related skin reactions. For patients who develop itching and significant skin irritation, a topical steroid cream might be considered. Topical lidocaine cream can also be considered for patients with intact skin and radiation related pain. If patients develop a significant skin reaction such as moist peeling of the skin, patients may be considered for a prescription topical lotion or cream to help accelerate healing and prevent the development of any skin infections. Other interventions that can be attempted include wound dressings such as ABD pads to reduce friction and irritation of the skin while keeping the topical creams on the skin. Please continue to use the recommended skin care regimen until told to do so by your radiation oncologist; the healing process can last several weeks after the radiation is finished, so you may be asked to continue using these interventions after your radiation is completed.
Your skin within the radiation area will be sensitive during and after treatment, so speak to your doctor about any creams or ointments you plan to put on your skin to make sure they won’t affect your treatment. Typically, patients are asked to remove any thick creams prior to treatment to avoid making the radiation reaction more intense. You will want to be gentle with your skin by avoiding significant friction when showering or bathing and pat the skin dry. It is also important to avoid extreme heat or cold temperatures directly to the skin, such as ice or heating packs, hot and cold water, and ice baths or saunas. Additionally, avoid skin products and/or perfumes that may irritate the skin and avoid deodorants that cause skin irritation, particularly if your skin is broken. You may also want to temporarily avoid shaving within the radiation areas given the sensitivity of the skin.
During and after radiation treatment, your skin may be more sensitive in the area you’ve received radiation than other areas of skin, so it is important to maintain a healthy skin care regimen. It is particularly important to protect your skin from the sun by avoiding exposure entirely, where possible, during treatment. After treatment, you will want to use high sun protection factor (SPF) sunscreen (usually SPF 50 or above) to protect your skin when outdoors for extended periods of time, to prevent sunburns.
While your skin remains sensitive during and after radiation, it is important to wear clothing that is comfortable and does not worsen the radiation related skin irritation. Make sure to discuss any questions that you may have with your treating radiation oncologist. Generally, patients are asked to wear loose fitting, breathable fabrics to avoid friction and/or rubbing against sensitive skin and allow aeration. You may also want to consider limiting the use of underwire bras, as they can cause extra irritation under the breast. Pay attention to where the breast straps sit against your chest wall and shoulder, as they can also cause irritation in areas where radiation is being directed towards the shoulder. For patients who have had a mastectomy and wear a breast prosthesis, pay close attention to the area where the prosthesis lays against the chest wall, as the presence of a prosthetic against the skin can lead to friction and irritation. Where possible, consider using a soft, lightweight prosthesis.
Patients may be receiving treatment in the summer time or otherwise when you may go to a pool to swim. Please talk to your doctor about specific recommendations if you would like to swim during or within 1-3 months after radiation therapy. In general, the skin irritation from the radiation can be worsened by the chemicals in the pool, therefore it is typically recommended that you avoid swimming entirely while the skin is irritated or broken. Additionally, if you notice any pain or irritation of the skin within the radiation area while swimming, stop immediately and speak to your radiation oncologist.
- Hair loss (more likely)
As radiation passes through the skin, it may also cause irritation to the hair follicles, resulting in hair loss. Therefore, anywhere the radiation enters or exists the body may be at risk for hair loss. For patients receiving breast cancer treatment, the most common area that hair is lost is under the armpit, but anywhere that is exposed to radiation along the chest wall and shoulder area can be affected. Hair loss can range from thinning of the hair to complete loss.
The hair loss can start within 1 to 2 weeks of starting treatment, but can also happen weeks to months later. The hair that is lost due to radiation therapy typically grows back, however in some cases, it goes away permanently. The hair may take several months to return, and when it does, it may be thinner or change in quality.
- Swelling, pain, tenderness
The breast is one of the main targets of the radiation used in reducing the risk of cancer recurrence. During the treatment, radiation can make it more difficult for the body to drain extra fluid from the breast. This may result in swelling of the breast and/or axillary (armpit) tissue. In addition to swelling, patients may also experience breast heaviness, tenderness, and soreness.
Breast swelling from radiation therapy can occur within the first 1-2 weeks of radiation therapy, but can occasionally start shortly after the radiation is completed. The swelling is typically transient and resolves on its own several weeks after completion of treatment.
If the breast remains uncomfortable, your radiation team may recommend you try over the counter analgesics such as ibuprofen or acetaminophen. If the symptoms persist even after completing therapy, your radiation oncologist may refer you to see a lymphedema specialist for an evaluation. They may be able to provide compression garments and/or lymphatic massage to help drain the extra fluid.
Of note, patients may also notice aches, twinges or sharp pains in the breast or chest area. These are typically related to the previous treatment you’ve received, including both surgery and radiation therapy, and the resulting breast swelling. These are usually mild and may continue for months or years after treatment is completed. However, they usually become less frequent and less intense over time.
- Muscle tightening (less likely)
After breast surgery, patients can have issues with the movement of their upper extremity. This can be more prominent when patients receive a mastectomy and/or have axillary surgery where many lymph nodes are removed. This can result in limitation in the range of motion of the arm. When this happens, patients are often given exercises by their breast surgeons to help restore the function of their arm to preoperative levels. It is important to have a functional range of motion of your arm before receiving radiation therapy because you are typically positioned with your arms above your head during your radiation treatments.
When patients receive radiation therapy, the treatment can cause the adjacent muscles to be irritated, resulting in muscle tightness. These muscles include those in the chest wall and shoulder area. When affected, this can cause further reductions in the range of motion of the arm, limitations in strength, and overall decreased functionality. Muscle tightness from radiation therapy typically starts 1-2 weeks into the radiation course, and may last several weeks after the radiation is completed.
To improve your muscle related symptoms, you may be asked to continue the arm related exercises you were given after your surgery. For those with significant limitations, your radiation oncologist may refer you to a physical therapist to get specific exercises about how to manage your arm mobility.
- Sore Throat (less likely)
For breast cancer patients receiving radiation to the lymph nodes above the clavicle, part of the radiation field may overlap with the esophagus. When that happens, you may develop a sore and/or dry throat, have pain when swallowing, or feel like your food is getting stuck in your throat when you swallow. Only a minority of patients who receive radiation to their lymph nodes eventually develop these symptoms, but if you do, please make your radiation team aware.
If you develop radiation irritation of the throat, it typically does not occur until 3-4 weeks into your radiation course, and can even start after the treatment is finished.
The treatment usually resolves without intervention within 1-2 weeks. For those whose symptoms are quite bothersome or interfering with their ability to eat, you may be suggested to try an over the counter pain medicine such as acetaminophen or ibuprofen; because of the discomfort, you may be asked to take these medicines in liquid form. Alternatively, you may be prescribed an oral solution to swallow, which coats the inside of your throat and makes it less painful, and can be helpful prior to eating.
Long term side effects
- Darkening/thickening of skin (more likely)
Once radiation is complete, you may notice skin changes that develop in the months or years after treatment. These changes may include changes in the color of the skin (called hyperpigmentation), changes in the skin texture, and the increased prominence of blood vessels (called telangectasias).
Patients may develop darkening of the skin within the radiation field after completing treatment. These changes are painless but can affect the cosmetic outcome of the breast after treatment. These effects can be more common with patients who have specific skin tones. Typically, these skin changes fade over time, but for some patients, they can last months to years, and occasionally indefinitely. These effects are not harmful but may be noticeable and can affect the cosmetic outcome. To mitigate these effects, your radiation oncologist will try to limit the radiation delivered to the skin and the total amount of skin involved with the treatment. At the same time, you can minimize your risk of these effects by following your physician’s skin care instructions. This typically includes using daily moisturizers throughout treatment and in the months immediately after treatment.
For patients who develop changes in skin texture or increased firmness of the skin, it typically occurs gradually, within the first few months, after the completion of therapy. You may notice the tightness when moving your upper extremities and noticing a pulling sensation. The changes can develop in addition to any changes that have occurred after a recent surgery. The goal of management is to reduce the risk of developing associated functional deficits as well as minimizing any associated discomfort. To accomplish this, patients are often referred to physical therapy, which can provide patients with an appropriate stretching routine to help maintain/regain the strength and flexibility of the involved joints. In rare cases, patients may benefit from injectional therapies (such as botox), hyperbaric oxygen, or pharmacologic agents (such as pentoxifylline and/or vitamin E).
Finally, after completing therapy, patients may develop small spider-like veins called telangiectasias. Telangiectasias are permanent but do not result in any adverse effect and are otherwise not bothersome or harmful. Typically, these areas are managed conservatively with observation. For cosmetic improvements, patients may consider using topical make up over the concerning areas. In rare cases, patients may also be referred for laser therapy.
- Scar tissue, breast size changes (more likely)
- Muscle tightening (less likely)
- Complications with breast reconstruction (more likely)
Once radiation therapy to the breast is complete, there can be changes to the breast that may affect how it feels and how it appears. The most significant changes typically happen within the first 6 months after completing treatment, but can continue to occur up to years later. Radiation therapy to the intact breast or to a reconstructed breast can cause the tissue to shrink or change shape compared to the opposite breast. The texture of the breast can also change, resulting in the skin feeling thicker, the breast feeling firmer, and the breast contour changing (such as the breast sitting higher on the chest wall) relative to how the breast was prior to radiation. When these changes occur after a breast reconstruction or tissue expander placement, the tissue can also feel hard and can result in pain and tightness when moving the arm.
Most of the time, patients feel these breast changes are manageable. Cosmetically, patients may use a breast insert in the bra to make their breast appear more symmetric. Patients may also be sent to physical therapy or lymphedema therapy if the related breast changes result in changes in range of motion of the arm or swelling of the soft tissue of the breast.
In a minority of cases, patients feel these changes are significant enough that they would like to have these changes addressed surgically. If so, please talk with your oncology team, including your breast surgeon and/or plastic surgeon, for recommendations about what can be done surgically to improve the cosmetic outcome.
- Breast and/or arm swelling (lymphedema)
Normally, fluid is brought to your tissues through your arteries, and is taken away by your veins and through the lymphatic system. When you undergo treatment for your breast cancer, your lymphatic system can be disrupted, resulting in less ability to remove fluid from your tissues. Also, when cancer is involving your lymph nodes or lymph nodes are removed as part of your cancer treatment, your remaining lymph nodes may not be able to handle removing all of the fluid, also resulting in fluid build up. This can result in a backup of fluid known as lymphedema.
Breast cancer patients are at highest risk for developing lymphedema within 2-3 years after completing breast cancer treatment. However, these symptoms can occur at any time along your breast cancer journey, from before receiving any treatment to many years after completion of all breast cancer treatment. The risk of developing lymphedema can increase if you have many lymph nodes removed at the time of your breast cancer surgery, are overweight or gain weight during your treatment, experience an infection of the breast or axillary area, overexposure to heat or development of a sunburn in the radiation area, or are otherwise delayed in seeking treatment for early symptoms.
When lymphedema occurs with breast cancer treatment, swelling can occur in the breast / chest wall area, arm, hand, shoulder. This swelling may also produce a sense of heaviness or fullness in the arm or tightness/stiffness when you move your shoulder, elbow, wrist, or hand. You may also notice that jewelry worn on the upper extremity, such as watches, rings, or bracelets, may be tight or difficult to put on or take off. This swelling can be transient, can fluctuate, or can persist permanently. If you notice asymmetric swelling of the arm that is on the same side you received breast cancer treatment, please contact your treating oncology team for an evaluation and recommendations.
To reduce your risk of developing lymphedema, your surgeon attempts to remove the fewest lymph nodes possible while still maintaining the best outcome for cancer control. This typically involves removing only a limited number of nodes at the time of your surgery; typically, this is called a sentinel lymph node biopsy (SLNBx), where the surgeon uses dyes or radioactive tracers to identify the most important lymph nodes and only removes those that were identified.
When a patient develops unilateral swelling, the first step is to have an evaluation by your oncology team. If there is any concern for lymphedema, you will usually be directed to a lymphedema specialist. These specialists can do measurements of the involved areas to formally diagnose lymphedema, but can also recommend an initial course of treatment. Treatments may consist of wearing a compression sleeve specific compression garment to help your body remove the excess fluid. You may also be asked to position your arm above your body, which helps by using gravity to help drain your arm. Sometimes, you may also be asked to put on a compression pump or undergo massage therapy to encourage the fluid to return to your body. Finally, please speak to your treatment team before engaging in upper extremity exercise. While engaging in healthy exercise and maintaining your upper extremity strength and range of motion can help lymphedema symptoms, heavy and/or repetitive lifting can cause symptoms to worsen. Your treatment team can help to determine what type of exercise is right for you.
- Rib fracture (less likely)
Radiation therapy typically passes through the bones and cartilage in your body to get to the breast, chest wall, and/or lymph nodes, where the radiation is most effective. The radiation can, however, result in causing the bones to be irritated or become weaker over many years.
For most patients, there are no noticeable changes that occur. Some patients may notice some discomfort, pain, and/or tenderness in the chest wall area. Sometimes, patients may also notice localized swelling in the area. Typically, these symptoms resolve on their own within days or weeks. To manage the discomfort, you may try over the counter analgesics such as tylenol or ibuprofen. If the symptoms do not resolve shortly, make sure to consult with your radiation oncologist for further guidance.
For others, the radiation can increase the risk of developing a fracture in the ribs or bones receiving radiation. These fractures are typically precipitated by some form of trauma to the chest wall, but the likelihood of developing a fracture is increased on the side that received radiation therapy compared to the opposite side. These fractures are treated similarly to any other rib fracture, with rest and limiting movements that make the pain worse. If you suspect you have developed a rib fracture, please speak to your physician for further assistance.
Rarely, radiation therapy delivered to treat your breast cancer can damage nerves located in the treatment area. This risk is usually very low for patients receiving a single course or radiation because nerves are typically quite resistant to radiation irritation and your doctors are able to keep the amount of radiation low enough to prevent injury. The most commonly affected nerves are in the lower neck, shoulders (above the clavicle), and in the armpit area. These nerves help to provide muscle function and sensation to the arm and shoulder.
If a patient were to develop radiation related nerve injury, this would typically occur years after your radiation treatment. Radiation induced nerve damage can result in symptoms in the arm and shoulder region, such as numbness, tingling, pain, and weakness. In severe cases, this may progress to paralysis. Of note, these symptoms would be limited only to the side in which you received radiation therapy.
If you develop nerve related symptoms, it is important to discuss this with your doctor, as they will need to make sure your symptoms are not related to other things that can happen in the neck and shoulder region. Sometimes, your evaluation may include tests such as getting a CT scan or MRI of the shoulder. Other times, you may be referred to a specialist, such as an orthopedic surgeon, neurologist, neurological surgeon, or physical therapist, to determine where the symptoms are coming from and to develop a plan to manage your symptoms.
- Shortness of breath/cough (less likely)
Patients receiving radiation for breast cancer typically have a small amount of lung receiving radiation. However, when the lymph nodes are treated in addition to the breast and/or chest wall, the amount of lung receiving radiation is increased. When too much of the lung receives radiation, it can lead to irritation of the lung itself. This is called pneumonitis.
When a patient develops pneumonitis, the symptoms do not typically start until between 1 and 6 months or more after the radiation is completed. The symptoms a patient may experience include coughing or shortness of breath, dry cough, and low grade fever, similar to what you might experience with a common cold. The symptoms are usually mild and resolve on their own. If you have any concern that you may be developing radiation pneumonitis, please notify your radiation oncologist.
In cases where a diagnosis is pursued, a patient may be sent for a chest x-ray or CT scan of the chest to understand how the lungs appear radiographically. These tests may identify irritation in the lungs where the radiation was most intense. Patients may be sent for pulmonary function tests (PFTs) to see how the lungs are functioning. Together, these tests can also help to identify other causes of breathing issues that can occur that do not involve radiation, such as COPD exacerbation or pneumonia. When identified, either based on clinical evaluation or imaging findings, patients with radiation pneumonitis can be asked to take over the counter ibuprofen or prescription steroids to help reduce the inflammation and improve the patient’s breathing.
- Heart Problems (less likely)
During your CT simulation, the heart is outlined so that it can be avoided during the radiation therapy. Your radiation oncologist will make every effort to minimize the radiation dose to the heart, as there are many different techniques to do so. However, during breast cancer radiation therapy, the heart can still receive radiation, which may result in an increased risk of developing heart disease in the future. The type of heart disease that can develop depends on the area of the heart receiving the radiation dose, and may include pericarditis (inflammation of the sac surrounding the heart), coronary artery disease (narrowing of the blood vessels supplying the heart), and/or issues with the valves between the heart chambers. Most commonly, patients who receive treatment to the left breast are at risk due to the position of the heart behind the left chest wall. Heart disease after radiation for breast cancer remains relatively rare, but when it does occur, it usually happens 5-10 years or more after receiving treatment.
The most important aspect toward minimizing heart effects of radiation involves your radiation oncologist identifying your heart during the simulation and avoiding it during your treatments. To do so, your physician may ask you to take a deep breath and hold the breath during treatment, which can change where the heart sits and move it away from the radiation beam. Other strategies may include changing the angle of the radiation beam or using advanced techniques such as “intensity modulation” to better distribute the radiation dose away from the heart.
Other health factors can also contribute to the development of heart disease. To optimize your heart health, it will be important to also adequately manage your blood pressure (hypertension), your blood sugar (diabetes), and your cholesterol, in addition to making sure you eat a healthy diet and get regular exercise.
- Second cancer (less likely)
After receiving radiation therapy, there is a risk that the radiation itself can cause a new cancer. This risk of developing a radiation induced cancer is very low and is outweighed by the benefit of the radiation reducing the risk of the cancer you are being treated for. In other words, the risk of the cancer coming back without the radiation is much higher than the risk of developing a cancer due to the radiation. These cancers do not appear immediately but most commonly take anywhere between 10 and 30 years to develop.
To limit the development of these radiation-induced cancers, we try to limit the patients receiving radiation to those who will benefit. Also, when developing a radiation plan, we try to limit the amount of your body exposed to the radiation. We do this by designing the radiation to pass through as few areas of the body as possible when traveling to its target. We also limit the areas of high radiation intensity to only the areas where it is necessary.
Patients themselves can also try to limit the development of new cancers by leading a healthy lifestyle, including eating a well-balanced diet, getting daily exercise, and limiting exposure to cancer causing agents such as smoking.
If a cancer develops due to radiation therapy, most commonly, it does not appear as a breast cancer, but rather a cancer of the connective tissue called a sarcoma. When identified, they can also be treated by your oncology team.
Copyright ASTRO
Privacy Policy
Terms of Use
251 18th Street South
8th Floor
Arlington, VA 22202
Telephone: 703-502-1550
www.astro.org
This section does not use cookies for tracking. By moving outside of this area, you will be moving to pages that store cookies to improve functionality.
Click "Continue" to proceed.